


Conceptualizing Healthcare Equity
Improving healthcare access and equity is reliant upon our understanding and measurement of social determinants of health that influence people’s capability, motivation, and opportunity to engage with healthcare services.1 Social determinants of health (SDOH) are broadly defined as the environment, or conditions, in which people work, live, learn, socialize, and continuously engage with that impact their quality of life and health.1-3 Equitable healthcare access can cover a number of health systems at various levels, such as insurance coverage, availability of healthcare providers, and distance/transportation to a health clinic.
Background
In the US over 24 million people are uninsured,4 with about 12% of adults reporting delaying seeking care due to cost.5 These numbers increase when examining sub-populations of the US; individuals in rural areas are more likely to utilize the emergency room department for medical care due to a shortage of primary care clinics, distance to preventative care, and inability to access teleservices.6 Historically marginalized communities, such as Black people, experience health disparities due to historic racist and discriminatory policies and practices that limit their ability to access healthcare services.7
While more midstream SDOHs (e.g., employment, living environment) are important to interact on, upstream SDOHs (e.g., public policies) directly shape the midstream SDOHs and inevitably individual-level factors impacting health.8 SDOH challenges the historical perception that health is solely impacted by an individual's personal choices (e.g., smoking tobacco) but by a broader system of interconnected influences.
Socio-Ecological Model (SEM)
Social science fields like public health, psychology, and social work have transitioned from an individual, biomedical perspective to one that includes the impact of social and structural determinants of health.1,9,10 Ecological models demonstrate that a person’s health is influenced by numerous interacting environmental systems that include a person’s immediate surroundings, the relationships between those systems, and larger societal norms and cultural aspects.11 These models are time-dependent and require researchers to assess the historical context of their target study population in addition to the current socio-political context. The socio-ecological model (SEM) is one framework to examine how multiple environments at varying proximities to a person can impact their access to healthcare, both discretely and overtly.12,13
The SEM is broken down into five major categories: structural, community, organizational, interpersonal, and individual. These categories provide the scaffolding to determine the measurements that are needed to assess influences impacting a person or group's ability to access healthcare services.

Using SEM to define Healthcare Equity Metrics
Having an understanding of the systems that influence a person’s behavior is crucial to developing health promotion interventions that address the root causes of a health problem.2,11,12,14 One way of gaining that understanding is by measuring those influences over a period of time to compare how influences may change. These metrics of health can provide data to support decision-making processes and goal-setting for future research or health promotion programs.2,15,16 Access to healthcare encompasses not only the availability of services but also affordability, proximity, cultural competence, insurance coverage, and the patient-provider relationship, making it impossible to capture the full picture with just one measure. SEM provides scaffolding to generate comprehensive interventions that can better tackle complex health issues.12
Structural systems are social policies, laws, and economic systems that impact population health outcomes. These are what are sometimes referred to as macrosystems in psychology or social work, and are often the furthest from a person or group in terms of interaction or proximity. Metrics that could capture structural-level factors impacting health are:
Medicaid/Medicare Expansion
State- or federal-level policy decision(s) that broaden eligibility for Medicaid and Medicare programs, increasing access to elderly, persons with disabilities, and low-income individuals. Data on expansion can be found at:
- Center for Medicare and Medicaid Services17
- Kaiser Family Foundation Medicaid Expansion Tracker18
- State Health Policy Database(s)
Health insurance coverage metrics
Measures the number of people with insurance coverage, including public, private, or a combination of both.
- The US Census Bureau,19 the Center for Disease Prevention and Controls National Center for Health Statistics,20 and the Kaiser Family Foundation offer national and state-level data for insurance coverage.
Health Equity Investments metrics
Measures financial/policy commitments made by governments, healthcare systems, or other institutions specifically aimed at addressing health disparities.
- Health Equity and Financial Protection Indicators21 for global maternal and child health
- The Health Equity Policy Tool22 is a framework to review current and proposed policies
- The Healthcare Equity Index23 assess LGBTQ-related policies and practices that impact health.
Community-level factors examine the relationship between organizations, organizations, and community members; and how those relationships build cultural norms within a defined area (i.e., geographical, cultural, internet) that influence health behaviors. These metrics are often highly informed by the target population or regional area, and can include:
Healthcare Facility Density, Proximity, and other Spatial Access to Healthcare Service Metrics
Measure the availability and accessibility of healthcare services relative to where people live, work, and engage in recreation, such as access to reliable transportation.
- Census data in combination with GIS mapping and health department registries can determine the predicted number of people a clinic serves in a given area.
Environmental Health Factors
Measure how attributes of our environment (i.e., parks, air quality), and exposures to those attributes, impact people’s health.
- Air Quality Index24 and Freshwater Quality Index25 can help measure pollutant levels
- Access to green spaces, walkability, and housing quality can be measured via local zoning maps/urban planning data and the US Department of Housing and Urban Development
Community Health Programs Metrics
Measure the number available community-based initiatives that support disease prevention, promote healthy living, and improve healthcare access.
- Local public health agency databases and Health Resources and Service Administration’s data warehouse provide a count of federally qualified health centers, WIC programs, and other health-focused initiatives.
The Complexity of Measuring Accessibility
Measuring spatial accessibility in order to assess spatial equity can be complex, and great consideration should be given to the method of measurement. One common method is the container method, which assesses the number of services available within a boundary such as a census tract. However, because container boundaries like census tracts are relatively arbitrary to people’s practical movement patterns, this method fundamentally constrains the notion of access being applied.26 Other methods that account for distance can be alternatives that do not as greatly constrain notions of access. These methods may account for distance by geographic distance, travel time, or travel cost.27 Learn more about these methods of measuring accessibility here.
Scale is also an important consideration. Common problems of scale, such as the modifiable areal unit problem (MAUP), mean that different results can be produced by working with the same data at different scales.28 Learn more about problems of scale here. Methods for measuring accessibility should be tailored to the research question being asked, and designed with consideration for common fallacies and spatial validity.
See also the Public Transit Equity guide for more information about measuring spatial accessibility.
Organizational-level factors include formal and informal rules and regulations an organization or institution (e.g., school, health clinics) expects people to follow, which impact a person’s willingness to engage in a health behavior. Typically, a singular system, such as a hospital or network of clinics, is assessed to determine potential factors influencing health, such as:
Workforce Diversity
Measures the representation and inclusion of individuals from various social identities (i.e., racial-ethnic, gender, education) in different organizational positions (i.e., clinical, administration, custodial).
- Organizational human resource data collected during hiring/onboarding, an internal audit, or self-reported demographics may be used
Access/Utilization of Telehealth
Measures the availability and use of remote healthcare services delivered via an app, text message, phone call, or other internet-based service.
- Electronic health records could indicate the number of people engaging in telehealth services
- The telehealth usability questionnaire29 is a 21-item measure assessing usefulness, ease of use, interface and interaction quality, reliability, and satisfaction.
Access to Timely Care
Measures a person’s ability to receive needed healthcare services in an appropriate and acceptable time frame.
- Surveying patients (i.e., “How often were you able to get an appointment for necessary care?”), collecting operational data (i.e., same-day appointment availability), and collecting observational data (i.e., observing wait times in an ER).
Interpersonal factors are the formal and informal social networks a person interacts with (e.g., family, friends, colleagues) that influence health behaviors. This may also include relationships with individual healthcare workers or physicians and is different from organizational factors that examine the larger clinic. Metrics to assess interpersonal factors can include:
Provider-Patient Trust Metrics
Measures patients’ confidence in their provider’s ability and willingness to act in their patient's best interest and provide quality care.
- Dugan et al.’s validated 5-item scale30 can identify trust in medical providers, health insurers, and other medical professionals
Family and Social Support Metrics
Measures the perceived availability and/or quality of support (i.e., emotional, informational, etc.) from family members, friends, or other social supports.
- The Multidimensional Scale of Perceived Social Support31 is a 12-item scale assessing support in friends, family, and significant others.
Experiences of Discrimination in Healthcare Metrics
Measures perceived and explicit experiences of being treated violently, unfairly, or differently based on personal characteristics (i.e., income, gender, racial-ethnic identity).
- The Discrimination in Medical Settings32 is a 7-item scale assessing prior experiences of mistreatment while receiving healthcare services.
Individual factors are a person's knowledge, beliefs, attitudes, and self-efficacy (e.g., skill) to engage in a specific health behavior. These are metrics that we are often familiar with seeing in health promotion literature and research. These metrics are still crucial to examine as they can provide insight into how all the other levels impact the individual, which can include:
Health Literacy Metrics
Measures a person’s ability to understand and use health information to make informed decisions about their care.
- The Brief Health Literacy Screening Tool33 is one way to assess health literacy.
- Additionally, you could ask “How often do you [need help reading/understand written] instructions from your doctor?” to quickly assess health literacy.
Preventative Screening Behaviors Metrics
Measures the frequency a person engages in one or more preventative screening behaviors (ex., bi-annual STI testing, Pap Smears, Colonoscopy)
- Self-reported measures can be used (e.g., Did you have a [insert screening behavior] in the last 12 months?), population data reports (e.g., the Behavioral Risk Factor Surveillance Survey), or electronic medical record data if possible.
Self-Reported Health Status Metrics
Measures a person’s perception of their health, which can be specified based on the research questions.
- The Self-Reported Health Questions (“How do you rate your health? Very good, Good, Moderate, Bad or Very bad?") is the most commonly used technique; however, multi-item questionnaires may provide more accurate and comprehensive data.34
By assessing factors across SEM levels, a comprehensive understanding of healthcare access barriers and facilitators can be developed, leading to more targeted and effective interventions.
Theory of Access
Theory of Access (Penchansky & Thomas, 1981)35 posits that healthcare access is a set of dimensions that describe the fit between patients and the larger healthcare system (i.e., clinicians, insurers, etc.) By optimizing these specific dimensions, we can improve healthcare access.
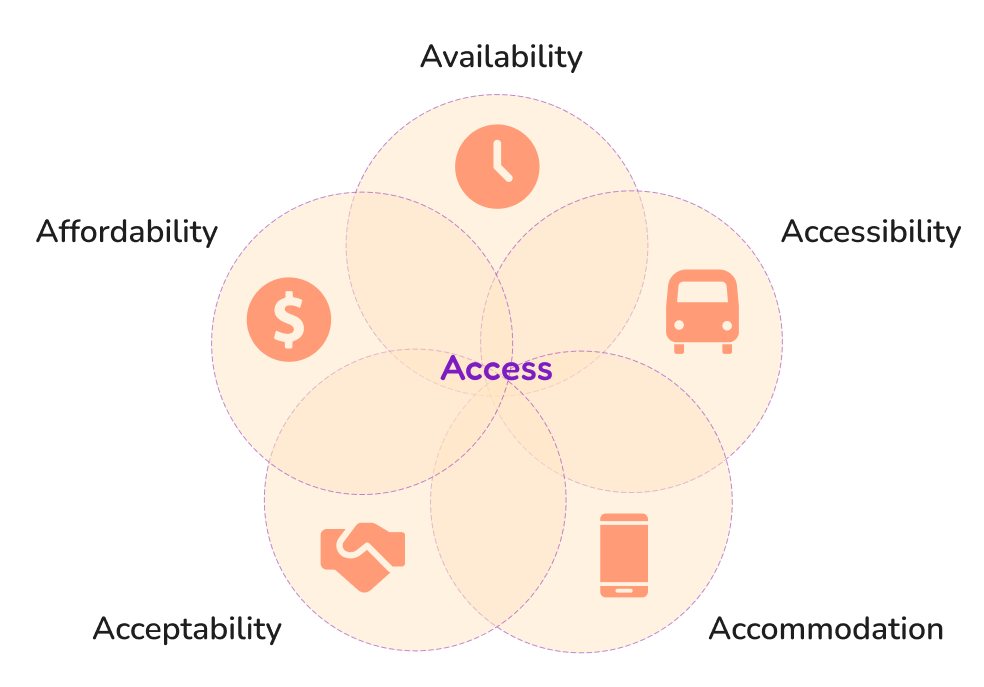
Table 1. Theory of Access dimensions
| Dimension | Example(s) |
|---|---|
| Availability | Healthcare resources (workforce, equipment, technology), wait times |
| Accessiblity | Centralized healthcare services, transportation, distance to nearest health service (i.e., ‘close to home’ care) |
| Accommodation | Healthcare’s organization and delivery of services, integrated services, telemedicine |
| Affordability | Insurance coverage, clinic funding for a specific service, indirect patient cost (i.e., transportation/lodging) |
| Acceptability | Relationships between patients and clinicians, characteristics of patients or clinicians, and patient preferences |
Check out Gao and Kolak’s (2019) paper36 on food access to see how the Theory of Access is used to support data collection and analysis! (see Table 2. Data Sources Measuring Healthcare Equity)
Apply Healthcare Equity Measures into Practice
Data collection and measurements are based on the research question at hand. Before measurement development can occur, it is crucial to have a basic understanding of the health problem of interest and factors that may impact that health problem. Reviewing the literature and existing data sources is the first step to measurement development. Table 2 presents a small sample of publicly available datasets or databases that collect health inequity data globally. Utilizing existing data can provide new insights into how health behaviors have changed and what may have caused those, and are particularly useful for measuring the success of public policies whose timeline for implementation may be delayed compared to an individual intervention.
Additionally, defining who the data is for and how it will be used is an important step in measurement development. Academic use of health equity measures are utilized to report prevalence data, how common a behavior or SDOH is, and evaluation of interventions. Community use of health equity measures may be utilized to leverage funding, raise awareness of a topic, and support calls for political action. Once the questions and the potential use for the metrics being collected has been defined, documentation of the methodology used to collect that data is essential. This is in part because anyone who wishes to replicate the study should be able to do so, but also this ensures:
- Transparency of the research
- Minimization of biases and harms
- Identification of potential limitations to the conclusions being drawn from the data
As the SEM demonstrates, multiple measures of healthcare access are needed to understand the complex relationships between an individual or group and their ability to access healthcare and health-related services. Multiple measures can provide a comprehensive understanding of the diverse factors that influence healthcare availability, quality, and fairness. The interconnectedness of different factors influencing health and how they may reinforce health disparities cannot be captured in a single measurement. Health disparities are deeply tied to broader SDOH. The SEM framework, with its multi-level focus, allows researchers to integrate and measure SDOH alongside more traditional health indicators (e.g., chronic conditions, mortality rates). This helps connect social, economic, and environmental factors to health outcomes, reinforcing the need for policies and programs that address these root causes.
Table 2. Data Sources Measuring Healthcare Equity
| Data Source | Description |
|---|---|
| World Health Organization Health Inequality Data Repository | A global database providing disaggregated health data across social and demographic factors to identify, analyze, and address health disparities through interactive tools and evidence-based policymaking. |
| National Center for Health Statistics | A collection of l statistics and health information to inform public health policy and research at the national level. |
| HealthData.gov | A US government open-data portal that provides access to a wide range of health-related datasets, statistics, and resources from federal agencies, supporting research, policy development, and innovation in public health. |
| Compendium of Federal Datasets Addressing Health Disparities | A collection of US government datasets focused on health inequities across different populations, such as race, ethnicity, socioeconomic status, geography, and other social determinants of health. |
| Mapping Medicare Disparities Tool | County and state-level data that identifies disparities in health outcomes, utilization, prevalence, and spending by race and ethnicity and geographic location. |
| Community health Status Indicators | County-level indicators of health outcomes, access and quality, health behaviors, social factors, and the physical environment. |
| Healthcare Cost and Utilization Project | National, state, and county-level data on diagnoses and procedures, discharge status, patient demographics, and charges for all patients regardless of payer. |
| Area Health Resource Files | National, state, and county data that compares population characteristics, health resources, and demographics. |
| Dartmouth Atlas of Health Care | Hospital, county, state, and region data on medical resource distribution, hospital care intensity, variations in care/ procedures, end-of-life care, and cost |
| Community Health Profiles | State and county-level data layer maps with demographic elements, SES, clinical care, health behaviors, and outcomes. |
| **State or County Health Department Data | Health-related information collected and maintained by local or state health departments, including data on diseases, health behaviors, environmental factors, and healthcare access, used to inform public health policies and interventions at the regional level. |
Note: This is not a comprehensive list, data sources listed here are all public access and free to use, however, there are databases with datasets that include health equity measures for a fee or require an application to use. Additionally, not all datasets previously available from government websites may still be available, or may no longer be updated regularly. See the SDOH Data Refuge for more information about archiving efforts and accessing datasets targeted for removal.
Resources
- Introductory Reading: “Introduction to Health Equity and Social Determinants of Health”
- The Institue for Healthcare Improvement Health and Well-Being Measurement and Approach Toolkit
- Health People 2030 Evidence-Based Resources
- The CDC’s Social Vulnerability Index
- The Health Resource and Service Administration clinician workforce database
- The Health Equity Organizational Assessment
- Kansas University Community Toolbox’s Assessing Community Need(s) and Resources
- Designing Healthy Environments at Work website
- Active Living Research Tools and Resources
About the Author

References
- Golden TL, Wendel ML. Public Health’s Next Step in Advancing Equity: Re-evaluating Epistemological Assumptions to Move Social Determinants From Theory to Practice. Front Public Health. 2020;8. doi:10.3389/fpubh.2020.00131
- Braveman P. Health disparities and health equity: concepts and measurement. Annu Rev Public Health. 2006;27:167-194. doi:10.1146/annurev.publhealth.27.021405.102103
- Healthy People 2030. Health Equity in Healthy People 2030. Accessed January 22, 2025. https://odphp.health.gov/healthypeople/priority-areas/health-equity-healthy-people-2030
- Cohen RA, Briones, Elizabeth M., Martinez, Micheal E. Health Insurance Coverage: Early Release of Estimates from the National Health Interview Survey, January–June 2024. National Center for Health Statistics (U.S.); 2024. doi:10.15620/cdc/170372
- Center for Disease Control and Prevention. NHIS-Adult Summary Health Statistics. September 25, 2018. Accessed February 14, 2025. https://wwwn.cdc.gov/NHISDataQueryTool/SHS_adult/index.html
- Rural Health Information Hub. Healthcare Access in Rural Communities Overview - Rural Health Information Hub. RHIhub. December 19, 2024. Accessed February 14, 2025. https://www.ruralhealthinfo.org/topics/healthcare-access
- Artiga S, Hill L, Published MP. How Present-Day Health Disparities for Black People Are Linked to Past Policies and Events. KFF; 2024. Accessed February 14, 2025. https://www.kff.org/racial-equity-and-health-policy/issue-brief/how-present-day-health-disparities-for-black-people-are-linked-to-past-policies-and-events/
- Islam MM. Social Determinants of Health and Related Inequalities: Confusion and Implications. Front Public Health. 2019;7. doi:10.3389/fpubh.2019.00011
- Ross WR. Promoting Health Equity: A New Challenge for Frontiers in Public Health. Front Public Health. 2013;1. doi:10.3389/fpubh.2013.00027
- Burton DC, Angele Kelly, Denise Cardo, et al. Principles of Health Equity Science for Public Health Action. Public Health Rep. 2023;139(3). Accessed February 10, 2025. https://journals-sagepub-com.revproxy.brown.edu/doi/10.1177/00333549231213162
- Bronfenbrenner U. Ecological systems theory (1992). In: Making Human Beings Human: Bioecological Perspectives on Human Development. Sage Publications Ltd; 2005:106-173.
- Stokols D. Translating Social Ecological Theory into Guidelines for Community Health Promotion. Am J Health Promot. 1996;10(4):282-298. doi:10.4278/0890-1171-10.4.282
- McLeroy KR, Bibeau D, Steckler A, Glanz K. An Ecological Perspective on Health Promotion Programs. Health Educ Q. 1988;15(4):351-377. doi:10.1177/109019818801500401
- Martin S, Dill J, Demeritte D, et al. A Scoping Review of Health Equity Interventions in Governmental Public Health. J Public Health Manag Pract. 2024;30(4):479. doi:10.1097/PHH.0000000000001947
- Quinn M, Robinson C, Forman J, Krein SL, Rosland AM. Survey Instruments to Assess Patient Experiences with Access and Coordination Across Healthcare Settings: Available and Needed Measures. Med Care. 2017;55(Suppl 7 1):S84-S91. doi:10.1097/MLR.0000000000000730
- Ganatra S, Khadke S, Kumar A, et al. Standardizing social determinants of health data: a proposal for a comprehensive screening tool to address health equity a systematic review. Health Aff Sch. 2024;2(12):qxae151. doi:10.1093/haschl/qxae151
- Centers for Medicare & Medicaid Services. Medicaid Enrollment Data Collected Through MBES. Medicaid.gov; https://www.medicaid.gov/medicaid/national-medicaid-chip-program-information/medicaid-chip-enrollment-data/medicaid-enrollment-data-collected-through-mbes
- Kaiser Family Foundation. Status of State Medicaid Expansion Decisions. KFF; 2026 https://www.kff.org/medicaid/status-of-state-medicaid-expansion-decisions/
- Keisler-Starkey, K., & Bunch, L. N. Health Insurance Coverage in the United States: 2023 (Current Population Reports P60-284). United States Census Bureau. 2024.
- National Center for Health Statistics. Health Insurance Coverage. CDC; 2023. https://www.cdc.gov/nchs/hus/topics/health-insurance-coverage.htm
- World Bank Group. Health Equity and Financial Protection Indicators. 2022. https://databank.worldbank.org/source/health-equity-and-financial-protection-indicators-(hefpi)#
- State Health and Value Strategies. Health Equity Policy Tool. SHVS; 2023. https://www.shvs.org/wp-content/uploads/2023/12/SHVS_Health-Equity-Policy-Tool.pdf
- Human Rights Campaign. Healthcare Equity Index 2024. HRC; 2024. https://www.hrc.org/resources/healthcare-equality-index
- AirNow. Air Quality Index (AQI) Basics. https://www.airnow.gov/aqi/aqi-basics/
- United States Environmental Protection Agency. Freshwater Quality. EPA; 2021. https://www.epa.gov/salish-sea/freshwater-quality#:~:text=The%20Freshwater%20Quality%20Index%20(WQI)%20is%20a%20tool%20developed%20by,Higher%20scores%20reflect%20cleaner%20water
- Talen, E., & Anselin, L. Assessing Spatial Equity: An Evaluation of Measures of Accessibility to Public Playgrounds. Environment and Planning A: Economy and Space. 1998;30(4): 595–613. https://doi.org/10.1068/a300595
- Long J. Modelling Accessibility. GIS&T BoK. 2017;Q3. doi:10.22224/gistbok/2017.3.7
- Mennis J. Problems of Scale and Zoning. GIS&T BoK. 2019;Q1. doi: 10.22224/gistbok/2019.1.2
- Parmanto B, Lewis AN, Graham KM, Bertolet MH. Development of the Telehealth Usability Questionnaire (TUQ). Int J Telerehabil. 2016;8(1):3-10. doi:10.5195/ijt.2016.6196
- Dugan E, Trachtenberg F, Hall MA. Development of abbreviated measures to assess patient trust in a physician, a health insurer, and the medical profession. BMC Health Serv Res. 2005;5(1):64. doi:10.1186/1472-6963-5-64
- Zimet GD, Dahlem NW, Zimet SG, Farley GK. The Multidimensional Scale of Perceived Social Support. Journal of Personality Assessment. 1988;52(1):30-41. doi:10.1207/s15327752jpa5201_2
- Wang VHC, Cuevas AG, Osokpo OH, et al. Discrimination in Medical Settings across Populations: Evidence From the All of Us Research Program. American Journal of Preventive Medicine. 2024;67(4):568-580. doi:10.1016/j.amepre.2024.05.018
- Wallston KA, Cawthon C, McNaughton CD, Rothman RL, Osborn CY, Kripalani S. Psychometric Properties of the Brief Health Literacy Screen in Clinical Practice. J Gen Intern Med. 2014;29(1):119-126. doi:10.1007/s11606-013-2568-0
- K. Van Ginneken J, Groenewold G. A Single- vs. Multi-Item Self-Rated Health Status Measure: A 21-Country Study. doi:10.2174/1874944501205010001
- Penchansky R, Thomas JW. The concept of access: definition and relationship to consumer satisfaction. Med Care. 1981;19(2):127-140. doi:10.1097/00005650-198102000-00001
- Gao I, Kolak M. Healthy Access for Healthy Places: A Multidimensional Food Access Measure. 2019. doi:10.48550/ARXIV.1912.11351









